

Volume 26, Issue 4 (Autumn 2020)
Intern Med Today 2020, 26(4): 316-331 |
Back to browse issues page



![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Ghajari E, Toozandehjani H, Nejat H. The Effectiveness of Marital Relationship Enrichment Training Based on Choice Theory, on Distress Tolerance of Women Recovered from Addiction. Intern Med Today 2020; 26 (4) :316-331
URL: http://imtj.gmu.ac.ir/article-1-3384-en.html
URL: http://imtj.gmu.ac.ir/article-1-3384-en.html



1- Department of Psychology, Neyshabur Branch, Islamic Azad University, Neyshabur, Iran.
2- Department of Psychology, Neyshabur Branch, Islamic Azad University, Neyshabur, Iran. ,hassan.toozandehjani1@gmail.com
3- Department of Psychology, Quchan Branch, Islamic Azad University, Quchan, Iran.
2- Department of Psychology, Neyshabur Branch, Islamic Azad University, Neyshabur, Iran. ,
3- Department of Psychology, Quchan Branch, Islamic Azad University, Quchan, Iran.
Keywords: Substance-related disorders, Drugs
Full-Text [PDF 5155 kb]
(2138 Downloads)
| Abstract (HTML) (3760 Views)
Full-Text: (3572 Views)
1. Introduction
n the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (2013), the presence of one of the cognitive, behavioral, and physiological symptoms are considered as an important feature of substance abuse disorder, but people, despite their awareness of significant problems of abuse, are not inclined to give it up. Most people in society consider substance abuse is a masculine phenomenon. However, women follow in the footsteps of men in this abyss so that statistics show a gradual increase in the number of women with substance abuse [1]. According to the latest World Drug Report, about 35 million people worldwide suffer from drug abuse disorders [2]. Recent UN reports on gender and drug abuse show that about 10% of drug users are women [3]. In Iran, the process of addiction moves from a “masculine” phenomenon to a “feminine and masculine” phenomenon [4]. Drug abuse in women is a multi-dimensional problem and several factors are effective in its occurrence and spread, besides, it has irreparable harm to the individual, family, and society [5].
Low distress tolerance can be considered as one of the underlying factors in the tendency toward various types of substance abuse. Distress tolerance is often defined as an individual’s self-report perceived ability to experience and tolerate negative emotional states [6] or as a person’s behavioral ability to persevere in goal-oriented behavior when experiencing emotional distress. Physically and behaviorally, distress tolerance is defined as the ability to tolerate distressing physiological states [7]. Currently, there is no comprehensive integrated distress tolerance model. Several authors have defined the latest possible structural models that attempt to integrate work on these and related structures [8]. Distress tolerance is increasingly seen as an important structure at the root of new insights into the onset and continuation of psychological trauma, and their prevention and treatment [9]. People with low distress tolerance engage in behavioral disorders in a misguided attempt to cope with their negative emotions and seek to alleviate their emotional pain by engaging in some destructive behaviors, such as substance abuse [10]. An emotion-driven coping strategy such as consuming alcohol and other substances may result in people getting rid of negative emotions quickly. This strategy is especially suitable for those who have low distress tolerance [11].
Continued use of cigarettes to reduce negative emotional states may be due to the difficulty of these people in enduring negative emotions [12]. Results of Daughters et al. study on 30 white and black American adolescents indicated that low distress tolerance increases the risk of alcoholism among whites, delinquent behavior among blacks, and symptoms of internalization disorders among women [13]. Moschak et al. showed that low distress tolerance was associated with high levels of cocaine use and impulsive behaviors [14]. Forouzanfar et al. concluded in a study that group counseling based on acceptance and commitment increased distress tolerance and decreased anxiety sensitivity of women dependent on substance abuse [15].
On the other hand, considering the importance of children’s upbringing, it is necessary to pay attention to the abnormal situation of women dependent on substance abuse and to consider solutions for the period after they quit their addiction. Therefore, family training is necessary to prevent harm to family life [16], and strengthening and stabilizing the family and satisfying the emotional and psychological needs of its members, especially spouses, are very important [17]. Children who live with a mother with substance abuse, experience severe psychological trauma, and suffer from many problems [18]. The longer children live with addicted parents, the more they suffer from physical illnesses and neurological disorders [19].
The quality of marital relationship plays an important role in the psychological health of family members and drug addicts, and if the inevitable conflicts of couples are severe, it will have devastating physical and psychological effects [20]. Marital relationship enrichment training based on “Choice Theory” is an educational approach to improve the marital relationship and its purpose is to help couples to be aware of reality, explore their positive and destructive behavior, develop empathy and intimacy and develop effective communication and problem-solving skills [21]. Fathollahzadeh et al. showed that the enrichment of marital life based on the “Choice Theory” would affect the quality of marital life and intimacy of couples [22]. Pourheidari et al. showed that relationship enrichment training would lead to couple adaptation [23]. Also, Agha Yousefi et al. in a study entitled “The Effect of Interpersonal Communication Enrichment Training on Marital Satisfaction of Addicted Spouses” concluded that interpersonal communication enrichment training could be effective in cases such as conflict resolution, self-expression, being more compliant, developing speaking skills, personal development skills, and changing spouse’s behavior [24].
The present study had shortcomings in several aspects. First, according to the researcher, there was no coherent study that has been published in the scientific community to examine the effect of enriching couples’ relationships on the distress tolerance of women who quit drugs. Second, a review of the research background indicates that the few studies conducted in this field have several limitations, including lack of follow-up to ensure the continued effectiveness of the intervention, impossibility of obtaining permission to enter women’s addiction camps or obtaining statistics on the number of women NA groups and the number of their members, and time constraints, which this study tried to eliminate such restrictions and problems. Third, studies showed that various strategies, including cognitive reconstruction and self-control strategies, were used in women who quit drugs, but relationships with husbands and life quality improvement education are new components that could be used in future research.
The most important perspective of this study was to prevent the children of these women from entering the cycle of crime and addiction. With the help of women who have given up drugs, we have saved their families and returned them to their families as guardians of their children. Women with substance abuse tend to become acquainted with drugs through close and intimate relationships, which can have potentially devastating consequences on their health. The most common psychological trauma experienced by men has been the experience of aggression and beatings by their peers, while women were the most victims of unwanted sexual behavior [25]. In women, health problems related to substance use are formed faster than men [25]. Given that today drug abuse has become an increasing problem among Iranian women who often belong to vulnerable groups in society, it is necessary to address this issue from various aspects (including the risk of exposure to prostitution, the birth of drug-addicted babies, and risk of having AIDS). By raising the level of distress tolerance in women who quit drugs, their children are given the chance to have a mother, a family, and a permanent home. These children have the opportunity to grow up healthy with the help of society and social institutions. By researching these variables, their role in the research background will be more prominent and will attract the attention of researchers and therapists in this field, and as a result, the opportunity to work on these variables will be provided. According to the above statements, this study aimed to determine the effectiveness of enriching couples’ relationships on increasing the anxiety tolerance of women who quit drugs Table 1.

2. Materials and Methods
The present study has a quasi-experimental design with pre-test, post-test, and follow-up and a control group. First, 40 women were selected from abstinent drug abusers, and according to the research method, which recommended at least 15 people for each group [26], 20 people were randomly assigned to the experimental group and 20 to the control group. The inclusion criteria for women entering the study were being married, being able to participate in training sessions with their husbands, lacking a mental or personality disorder of either couple (this criterion was assessed through a mental health interview), not having husbands addicted to drugs, and lacking a specific illness or pain that prevents them from attending sessions. The exclusion criteria were as follows: more than three absences from the sessions, relapse to drug use during the study, and relapse to drug use by spouses who had previously been addicted to drugs.
After the proposal was approved and the code of ethics (IR.IAU.NEYSHABUR.REC.1398.002) was obtained, a list of volunteers was prepared by referring to the women’s addiction treatment camp. Then, written consent was obtained from the volunteers to participate in the research, and finally, 40 people were selected and randomly assigned to the experimental and control groups.
In the next step, all subjects were assessed. The subjects in the experimental group participated in the marital relationship enrichment sessions, and the subjects in the control group remained on the waiting list. At the end of the training period and after three months, post-test and follow-up tests were taken, respectively. Multivariate ANOVA with repeated measures was used to analyze the data. The above analyzes were performed in SPSS V. 24.
The marital relationship enrichment was based on the “Choice Theory” and on the model of Duba, Graham, Britzman, and Minatra (2009) through the WDEP system in which W represents “wants”, D represents “doing”, E represents “evaluation”, and P represents “planning”, which was performed in three stages of six 90-min sessions as follows:
The following tools were used in this study
Distress Tolerance Scale: This questionnaire was designed by Simmons and Gaher (2005) which includes 15 questions. Items on this scale measure distress tolerance based on an individual’s abilities to cope with emotional distress, mental assessment of distress, attention to negative emotions if they occur, and regulatory measures to relieve distress. Alpha coefficients in the main version of this questionnaire were reported from 0.70 to 0.82 for subscales and 0.82 for the whole scale. It also had good criterion validity and convergence [11]. In Esmaili Nasab et al.’s study, the Cronbach α of the total scale was 86% [27]. Azizi, Mirzaei, and Shams reported a Cronbach α of 67% of the questionnaire and 79% of the retest validity of this questionnaire. The cut-off point of the distress tolerance scale was less than 28. A score higher than this indicated high distress tolerance. Scoring was in the form of a 5-point Likert-type scale, which was scored from “complete agreement” to “complete disagreement”. The validity coefficient (Cronbach α) in the Iranian sample was reported to be 0.82.
3. Results
Table 2 shows the demographic results of the subjects.

Table 3 provides descriptive information corresponding to the research variables.

Results showed that marital relationship enrichment improved the situation of women participating in the study. The mean distress tolerance in the experimental group in the pre-test stage increased from 34.533 to 42.80 in the post-test stage and the follow-up stage the mean reached 42.533. In the control group, the mean distress tolerance was close to each other in almost all three stages and there were no significant changes in this regard.
The research hypothesized that marital relationship enrichment affected the tolerance of women released from drug abuse. To evaluate the significant difference between distress tolerance scores in the experimental and control groups, repeated-measures ANOVA was used. Before performing the repeated measures ANOVA, to comply with the test assumptions, the results of the Box’s M, Mauchly’s sphericity, and Levene’s test were checked (Table 4).

Since the Box’s M test result was not significant for any of the research variables, the condition of homogeneity of variance-covariance matrices was observed. Also, the non-significance of any of the variables in Levene’s test showed that the condition of equality of variance between groups was observed and the amount of variance of error of dependent variables was equal in all groups. Finally, the results of the Mauchly’s sphericity test showed that this test was not significant for any of the variables, and therefore the assumption of the equality of variances within the subjects was observed.
Results indicated that the significance level for the control and experimental groups was more than 0.05, so the null hypothesis of the test was not rejected (P>0.05) (Table 4).
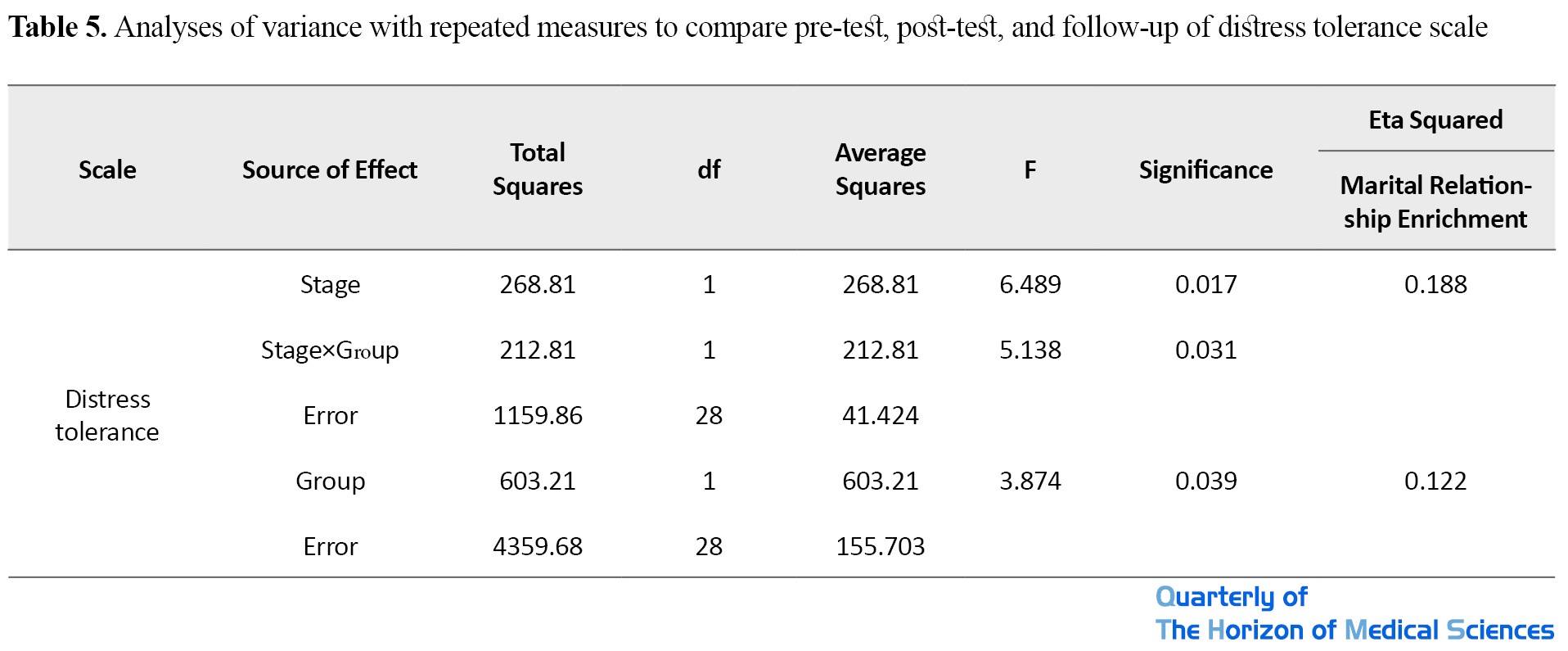
The results, considering the significance of the stage effect, indicated a significant difference between the mean of pre-test, post-test, and follow-up of the distress tolerance scales of the experimental group and the control group (P<0.05). Also, the significance of the interaction between the stages and the experimental group in the mentioned variables indicated that in the post-test and follow-up stages, the average scores of the experimental groups were significantly higher than those of the control group (Table 5).
Bonferroni post hoc test was used for paired comparison of the groups.
The results show that the scores of distress tolerance variables in the experimental group and the control group in the pre-test and post-test stages were significantly different from each other and women participating in the study in two variables improved due to the enrichment of marital relationships (Table 6).
.jpg)
4. Discussion
The results of testing the research hypothesis that marital relationship enrichment affected the distress tolerance of women recovered from drug abuse indicated that this training made a significant difference in the distress tolerance of the experimental and control groups in the post-test and follow-up stages. These results were consistent with the results of Moschak et al. (2017), Daughters et al. (2009), and Forouzanfar et al. (2017).
The results can be explained as follows. First of all, the core of training for enriching marital relationships based on the “Choice Theory” emphasizes “focusing on one’s behavior”, “control and choice”, “creating and accepting responsibility”, “accepting the realities of life and not denying them”, “the ability to satisfy basic needs and learn the psychology of self-control”, “assessing behavior for right or wrong”, and “judging self-behavior and self-control”. So “Choice Theory” can affect the distress tolerance of women recovered from addiction because distress tolerance is a psychological construct that means “the ability of individuals to resist negative emotions”.
As Simons and Gaher (2005) argued, people with low distress tolerance, cannot bear emotion and handle their distress, so these people do not accept the existence of emotion and are ashamed of it, because they underestimate their ability to cope with emotions. In the training sessions of marital relationship enrichment based on the “Choice Theory”, individuals learn skills based on “accepting reality without trying to change” and learn that pain and distress cannot be eliminated or avoided. Rather, the ability to accept unchangeable reality leads to a reduction in suffering. People who cannot rationally manage the pressures of married life and use avoidance methods instead of focusing on and accepting problems to find better solutions are more likely to feel helpless and less powerful as the pressures and stresses of married life intensify. This will increase avoidance practices in dealing with problems. Besides, people learn that if they do not try to change themselves, impulsive actions will replace the effort to make the desired changes.
As Klog 2004 points out, what’s most influential in distress tolerance is the relationship and environmental support. Because the experimental group interventions took place privately and in the counseling center, the researcher could create a friendly and empathetic atmosphere to facilitate the establishment of a therapeutic alliance with the couple. The relationship between the researcher and the participants paved the way for gaining trust. In this way, they were helped to believe that the actual healing process would be beneficial to them. Based on the trust created in gaining a sense of belonging in the relationship, the researcher helped the couple to make choices that were satisfactory to them, choices that were acceptable and enjoyable for both of them.
Women recovered from addiction generally do not have anyone in their qualitative world or someone with whom they could communicate satisfactorily. To make the treatment more successful, the researcher tried to fit into the qualitative world of the participants by creating a relationship. The researcher believes that the intervention could effectively enter the qualitative world of individuals. Based on this relationship with the researcher, couples could learn how to be intimate with the people who need them.
5. Conclusions
Because of the growing trend of women’s addiction in the country, appropriate education is a necessity. Therefore, it is recommended that effective steps be taken to improve the distress tolerance of women released from addiction, by marital relationship enrichment.
The limitations of the present study were related to the narrative honesty and behavioral and moral problems of women recovered from addiction. The lack of personal security of women and the obsession that was formed for them during drug consumption may result in invalid information obtained in filling out the questionnaires. The issue of honesty and behavioral and moral problems was so prominent that after personal satisfaction, they were among the most important factors in sample selection in the research.
Also, the researcher had to wait until the holding of NA open group meetings to encourage women recovered from addiction to participate in the research, which prolonged the research process.
Also, because of the lack of familiarity of couples with the researcher and lack of trust in him, it was necessary to spend considerable time to establish a relationship and to form a sense of trust.
The researcher’s limitations were undoubtedly included in this research. These included differences in the social class of the researcher and the participants. Especially since many members of NA groups did not have a good attitude towards psychologists and believed that psychologists could not understand their problems and improve them.
It is suggested that studies on male subjects be performed in future research. It would also be useful to focus on the effectiveness of other treatment approaches in future research to provide a clearer picture of the effectiveness of treatment methods, and marital relationship enrichment training packages be prepared in the form of books, pamphlets, brochures, or CDs and provided to NA groups.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Neyshabur Branch, Islamic Azad University (Code: IR.IAU.NEYSHABUR.REC.1398.002).
Funding
The present paper was extracted from the PhD. thesis of the first author, Department of Psychology, Neyshabur Branch, Islamic Azad University, Neyshabur.
Authors' contributions
Execution of protocol, execution, and compilation of manuscript: Elham Ghajari; Main idea and the final review of the article: Hassan ToozandehJani; Collect data, and analysis: Hamid Nejat.
Conflicts of interest
The authors declared no conflict of interest.
Acknowledgements
We thank and appreciate all addiction treatment clinics, especially the Addicted Neishabourian women who quit as well as all people who quit drugs Drugs helped researchers in this study.
References
n the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (2013), the presence of one of the cognitive, behavioral, and physiological symptoms are considered as an important feature of substance abuse disorder, but people, despite their awareness of significant problems of abuse, are not inclined to give it up. Most people in society consider substance abuse is a masculine phenomenon. However, women follow in the footsteps of men in this abyss so that statistics show a gradual increase in the number of women with substance abuse [1]. According to the latest World Drug Report, about 35 million people worldwide suffer from drug abuse disorders [2]. Recent UN reports on gender and drug abuse show that about 10% of drug users are women [3]. In Iran, the process of addiction moves from a “masculine” phenomenon to a “feminine and masculine” phenomenon [4]. Drug abuse in women is a multi-dimensional problem and several factors are effective in its occurrence and spread, besides, it has irreparable harm to the individual, family, and society [5].
Low distress tolerance can be considered as one of the underlying factors in the tendency toward various types of substance abuse. Distress tolerance is often defined as an individual’s self-report perceived ability to experience and tolerate negative emotional states [6] or as a person’s behavioral ability to persevere in goal-oriented behavior when experiencing emotional distress. Physically and behaviorally, distress tolerance is defined as the ability to tolerate distressing physiological states [7]. Currently, there is no comprehensive integrated distress tolerance model. Several authors have defined the latest possible structural models that attempt to integrate work on these and related structures [8]. Distress tolerance is increasingly seen as an important structure at the root of new insights into the onset and continuation of psychological trauma, and their prevention and treatment [9]. People with low distress tolerance engage in behavioral disorders in a misguided attempt to cope with their negative emotions and seek to alleviate their emotional pain by engaging in some destructive behaviors, such as substance abuse [10]. An emotion-driven coping strategy such as consuming alcohol and other substances may result in people getting rid of negative emotions quickly. This strategy is especially suitable for those who have low distress tolerance [11].
Continued use of cigarettes to reduce negative emotional states may be due to the difficulty of these people in enduring negative emotions [12]. Results of Daughters et al. study on 30 white and black American adolescents indicated that low distress tolerance increases the risk of alcoholism among whites, delinquent behavior among blacks, and symptoms of internalization disorders among women [13]. Moschak et al. showed that low distress tolerance was associated with high levels of cocaine use and impulsive behaviors [14]. Forouzanfar et al. concluded in a study that group counseling based on acceptance and commitment increased distress tolerance and decreased anxiety sensitivity of women dependent on substance abuse [15].
On the other hand, considering the importance of children’s upbringing, it is necessary to pay attention to the abnormal situation of women dependent on substance abuse and to consider solutions for the period after they quit their addiction. Therefore, family training is necessary to prevent harm to family life [16], and strengthening and stabilizing the family and satisfying the emotional and psychological needs of its members, especially spouses, are very important [17]. Children who live with a mother with substance abuse, experience severe psychological trauma, and suffer from many problems [18]. The longer children live with addicted parents, the more they suffer from physical illnesses and neurological disorders [19].
The quality of marital relationship plays an important role in the psychological health of family members and drug addicts, and if the inevitable conflicts of couples are severe, it will have devastating physical and psychological effects [20]. Marital relationship enrichment training based on “Choice Theory” is an educational approach to improve the marital relationship and its purpose is to help couples to be aware of reality, explore their positive and destructive behavior, develop empathy and intimacy and develop effective communication and problem-solving skills [21]. Fathollahzadeh et al. showed that the enrichment of marital life based on the “Choice Theory” would affect the quality of marital life and intimacy of couples [22]. Pourheidari et al. showed that relationship enrichment training would lead to couple adaptation [23]. Also, Agha Yousefi et al. in a study entitled “The Effect of Interpersonal Communication Enrichment Training on Marital Satisfaction of Addicted Spouses” concluded that interpersonal communication enrichment training could be effective in cases such as conflict resolution, self-expression, being more compliant, developing speaking skills, personal development skills, and changing spouse’s behavior [24].
The present study had shortcomings in several aspects. First, according to the researcher, there was no coherent study that has been published in the scientific community to examine the effect of enriching couples’ relationships on the distress tolerance of women who quit drugs. Second, a review of the research background indicates that the few studies conducted in this field have several limitations, including lack of follow-up to ensure the continued effectiveness of the intervention, impossibility of obtaining permission to enter women’s addiction camps or obtaining statistics on the number of women NA groups and the number of their members, and time constraints, which this study tried to eliminate such restrictions and problems. Third, studies showed that various strategies, including cognitive reconstruction and self-control strategies, were used in women who quit drugs, but relationships with husbands and life quality improvement education are new components that could be used in future research.
The most important perspective of this study was to prevent the children of these women from entering the cycle of crime and addiction. With the help of women who have given up drugs, we have saved their families and returned them to their families as guardians of their children. Women with substance abuse tend to become acquainted with drugs through close and intimate relationships, which can have potentially devastating consequences on their health. The most common psychological trauma experienced by men has been the experience of aggression and beatings by their peers, while women were the most victims of unwanted sexual behavior [25]. In women, health problems related to substance use are formed faster than men [25]. Given that today drug abuse has become an increasing problem among Iranian women who often belong to vulnerable groups in society, it is necessary to address this issue from various aspects (including the risk of exposure to prostitution, the birth of drug-addicted babies, and risk of having AIDS). By raising the level of distress tolerance in women who quit drugs, their children are given the chance to have a mother, a family, and a permanent home. These children have the opportunity to grow up healthy with the help of society and social institutions. By researching these variables, their role in the research background will be more prominent and will attract the attention of researchers and therapists in this field, and as a result, the opportunity to work on these variables will be provided. According to the above statements, this study aimed to determine the effectiveness of enriching couples’ relationships on increasing the anxiety tolerance of women who quit drugs Table 1.
2. Materials and Methods
The present study has a quasi-experimental design with pre-test, post-test, and follow-up and a control group. First, 40 women were selected from abstinent drug abusers, and according to the research method, which recommended at least 15 people for each group [26], 20 people were randomly assigned to the experimental group and 20 to the control group. The inclusion criteria for women entering the study were being married, being able to participate in training sessions with their husbands, lacking a mental or personality disorder of either couple (this criterion was assessed through a mental health interview), not having husbands addicted to drugs, and lacking a specific illness or pain that prevents them from attending sessions. The exclusion criteria were as follows: more than three absences from the sessions, relapse to drug use during the study, and relapse to drug use by spouses who had previously been addicted to drugs.
After the proposal was approved and the code of ethics (IR.IAU.NEYSHABUR.REC.1398.002) was obtained, a list of volunteers was prepared by referring to the women’s addiction treatment camp. Then, written consent was obtained from the volunteers to participate in the research, and finally, 40 people were selected and randomly assigned to the experimental and control groups.
In the next step, all subjects were assessed. The subjects in the experimental group participated in the marital relationship enrichment sessions, and the subjects in the control group remained on the waiting list. At the end of the training period and after three months, post-test and follow-up tests were taken, respectively. Multivariate ANOVA with repeated measures was used to analyze the data. The above analyzes were performed in SPSS V. 24.
The marital relationship enrichment was based on the “Choice Theory” and on the model of Duba, Graham, Britzman, and Minatra (2009) through the WDEP system in which W represents “wants”, D represents “doing”, E represents “evaluation”, and P represents “planning”, which was performed in three stages of six 90-min sessions as follows:
The following tools were used in this study
Distress Tolerance Scale: This questionnaire was designed by Simmons and Gaher (2005) which includes 15 questions. Items on this scale measure distress tolerance based on an individual’s abilities to cope with emotional distress, mental assessment of distress, attention to negative emotions if they occur, and regulatory measures to relieve distress. Alpha coefficients in the main version of this questionnaire were reported from 0.70 to 0.82 for subscales and 0.82 for the whole scale. It also had good criterion validity and convergence [11]. In Esmaili Nasab et al.’s study, the Cronbach α of the total scale was 86% [27]. Azizi, Mirzaei, and Shams reported a Cronbach α of 67% of the questionnaire and 79% of the retest validity of this questionnaire. The cut-off point of the distress tolerance scale was less than 28. A score higher than this indicated high distress tolerance. Scoring was in the form of a 5-point Likert-type scale, which was scored from “complete agreement” to “complete disagreement”. The validity coefficient (Cronbach α) in the Iranian sample was reported to be 0.82.
3. Results
Table 2 shows the demographic results of the subjects.
Table 3 provides descriptive information corresponding to the research variables.
Results showed that marital relationship enrichment improved the situation of women participating in the study. The mean distress tolerance in the experimental group in the pre-test stage increased from 34.533 to 42.80 in the post-test stage and the follow-up stage the mean reached 42.533. In the control group, the mean distress tolerance was close to each other in almost all three stages and there were no significant changes in this regard.
The research hypothesized that marital relationship enrichment affected the tolerance of women released from drug abuse. To evaluate the significant difference between distress tolerance scores in the experimental and control groups, repeated-measures ANOVA was used. Before performing the repeated measures ANOVA, to comply with the test assumptions, the results of the Box’s M, Mauchly’s sphericity, and Levene’s test were checked (Table 4).
Since the Box’s M test result was not significant for any of the research variables, the condition of homogeneity of variance-covariance matrices was observed. Also, the non-significance of any of the variables in Levene’s test showed that the condition of equality of variance between groups was observed and the amount of variance of error of dependent variables was equal in all groups. Finally, the results of the Mauchly’s sphericity test showed that this test was not significant for any of the variables, and therefore the assumption of the equality of variances within the subjects was observed.
Results indicated that the significance level for the control and experimental groups was more than 0.05, so the null hypothesis of the test was not rejected (P>0.05) (Table 4).
The results, considering the significance of the stage effect, indicated a significant difference between the mean of pre-test, post-test, and follow-up of the distress tolerance scales of the experimental group and the control group (P<0.05). Also, the significance of the interaction between the stages and the experimental group in the mentioned variables indicated that in the post-test and follow-up stages, the average scores of the experimental groups were significantly higher than those of the control group (Table 5).
Bonferroni post hoc test was used for paired comparison of the groups.
The results show that the scores of distress tolerance variables in the experimental group and the control group in the pre-test and post-test stages were significantly different from each other and women participating in the study in two variables improved due to the enrichment of marital relationships (Table 6).
4. Discussion
The results of testing the research hypothesis that marital relationship enrichment affected the distress tolerance of women recovered from drug abuse indicated that this training made a significant difference in the distress tolerance of the experimental and control groups in the post-test and follow-up stages. These results were consistent with the results of Moschak et al. (2017), Daughters et al. (2009), and Forouzanfar et al. (2017).
The results can be explained as follows. First of all, the core of training for enriching marital relationships based on the “Choice Theory” emphasizes “focusing on one’s behavior”, “control and choice”, “creating and accepting responsibility”, “accepting the realities of life and not denying them”, “the ability to satisfy basic needs and learn the psychology of self-control”, “assessing behavior for right or wrong”, and “judging self-behavior and self-control”. So “Choice Theory” can affect the distress tolerance of women recovered from addiction because distress tolerance is a psychological construct that means “the ability of individuals to resist negative emotions”.
As Simons and Gaher (2005) argued, people with low distress tolerance, cannot bear emotion and handle their distress, so these people do not accept the existence of emotion and are ashamed of it, because they underestimate their ability to cope with emotions. In the training sessions of marital relationship enrichment based on the “Choice Theory”, individuals learn skills based on “accepting reality without trying to change” and learn that pain and distress cannot be eliminated or avoided. Rather, the ability to accept unchangeable reality leads to a reduction in suffering. People who cannot rationally manage the pressures of married life and use avoidance methods instead of focusing on and accepting problems to find better solutions are more likely to feel helpless and less powerful as the pressures and stresses of married life intensify. This will increase avoidance practices in dealing with problems. Besides, people learn that if they do not try to change themselves, impulsive actions will replace the effort to make the desired changes.
As Klog 2004 points out, what’s most influential in distress tolerance is the relationship and environmental support. Because the experimental group interventions took place privately and in the counseling center, the researcher could create a friendly and empathetic atmosphere to facilitate the establishment of a therapeutic alliance with the couple. The relationship between the researcher and the participants paved the way for gaining trust. In this way, they were helped to believe that the actual healing process would be beneficial to them. Based on the trust created in gaining a sense of belonging in the relationship, the researcher helped the couple to make choices that were satisfactory to them, choices that were acceptable and enjoyable for both of them.
Women recovered from addiction generally do not have anyone in their qualitative world or someone with whom they could communicate satisfactorily. To make the treatment more successful, the researcher tried to fit into the qualitative world of the participants by creating a relationship. The researcher believes that the intervention could effectively enter the qualitative world of individuals. Based on this relationship with the researcher, couples could learn how to be intimate with the people who need them.
5. Conclusions
Because of the growing trend of women’s addiction in the country, appropriate education is a necessity. Therefore, it is recommended that effective steps be taken to improve the distress tolerance of women released from addiction, by marital relationship enrichment.
The limitations of the present study were related to the narrative honesty and behavioral and moral problems of women recovered from addiction. The lack of personal security of women and the obsession that was formed for them during drug consumption may result in invalid information obtained in filling out the questionnaires. The issue of honesty and behavioral and moral problems was so prominent that after personal satisfaction, they were among the most important factors in sample selection in the research.
Also, the researcher had to wait until the holding of NA open group meetings to encourage women recovered from addiction to participate in the research, which prolonged the research process.
Also, because of the lack of familiarity of couples with the researcher and lack of trust in him, it was necessary to spend considerable time to establish a relationship and to form a sense of trust.
The researcher’s limitations were undoubtedly included in this research. These included differences in the social class of the researcher and the participants. Especially since many members of NA groups did not have a good attitude towards psychologists and believed that psychologists could not understand their problems and improve them.
It is suggested that studies on male subjects be performed in future research. It would also be useful to focus on the effectiveness of other treatment approaches in future research to provide a clearer picture of the effectiveness of treatment methods, and marital relationship enrichment training packages be prepared in the form of books, pamphlets, brochures, or CDs and provided to NA groups.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Neyshabur Branch, Islamic Azad University (Code: IR.IAU.NEYSHABUR.REC.1398.002).
Funding
The present paper was extracted from the PhD. thesis of the first author, Department of Psychology, Neyshabur Branch, Islamic Azad University, Neyshabur.
Authors' contributions
Execution of protocol, execution, and compilation of manuscript: Elham Ghajari; Main idea and the final review of the article: Hassan ToozandehJani; Collect data, and analysis: Hamid Nejat.
Conflicts of interest
The authors declared no conflict of interest.
Acknowledgements
We thank and appreciate all addiction treatment clinics, especially the Addicted Neishabourian women who quit as well as all people who quit drugs Drugs helped researchers in this study.
References
- Sadock BJ, Sadock VA. Kaplan and Sadock's synopsis of psychiatry: Behavioral sciences, clinical psychiatry [N. Pourafkari, Persian trans]. Tehran: Shahrab, Ayandesazan; 2003. http://opac.nlai.ir/opac-prod/bibliographic/698442
- United Nations. World drug report 2019 [Internet]. 2019 [Updated 2019 June 19]. Available from: https://wdr.unodc.org/wdr2019/
- United Nations. World drug report 2017 [Internet]. 2017 [Updated 2017 June 16]. Available from: https://www.unodc.org/wdr2017/index.html
- Abasi I, Mohammadkhani P. Family risk factors among women with addiction-related problems: An Integrative review. International Journal of High Risk Behaviors and Addiction. 2016; 5(2):e27071. [DOI:10.5812/ijhrba.27071] [PMID] [PMCID]
- Qasemi Roshan E. [From women’s addiction to family disorder (Persian)]. Women’s Strategic Studies Quarterly. 2004; 22:130-51. https://www.sid.ir/fa/journal/ViewPaper.aspx?id=198095
- Simons J, Gaher R. The distress tolerance scale: Development and validation of a self-report measure. Motivation and Emotion. 2005; 29(2):83-102. [DOI:10.1007/s11031-005-7955-3]
- MacKillop J, de Wit H. The Wiley-Blackwell handbook of addiction psychopharmacology. Hoboken: John Wiley & Sons; 2013. [DOI:10.1002/9781118384404]
- Bernstein A, Zvolensky MJ, Vujanovic AA, Moos R. Integrating anxiety sensitivity, distress tolerance, andiscomfort intolerance: A hierarchical model of affect sensitivity and tolerance. Behavior Therapy. 2009; 40(3):291-301. [DOI:10.1016/j.beth.2008.08.001] [PMID]
- Zvolensky MJ, Bernstein A, Vujanovic AA. Distress tolerance: Theory, research, and clinical application. New York: Guilford Press; 2011. https://books.google.com/books?id=70zBvWRE1PcC&dq
- Keough ME, Riccardi CJ, Timpano KR, Mitchell MA, Schmidt NB. Anxiety symptomatology: The association with distress tolerance and anxiety sensitivity. Behavior Therapy. 2010; 41(4):567-74. [DOI:10.1016/j.beth.2010.04.002] [PMID] [PMCID]
- Azizi A, Mirzaei A, Shams J. [Correlation between distress tolerance and emotional regulation with students smoking dependence (Persian)]. Hakim Health Systems Research Journal. 2010; 13(1):13-8. http://hakim.hbi.ir/article-1-608-fa.html
- Brown RA, Lejuez, CW, Kahler CW, Strong DR. Distress tolerance and duration of past smoking cessation attempts. Journal of Abnormal Psychology. 2002; 111(1):180-5. [DOI:10.1037/0021-843X.111.1.180] [PMID]
- Daughters SB, Reynolds EK, MacPherson L, Kahler CW, Danielson CK, Zvolensky M, et al. Distress tolerance and early adolescent externalizing and internalizing symptoms: The moderating role of gender and ethnicity. Behaviour Research and Therapy. 2009; 47(3):198-205. [DOI:10.1016/j.brat.2008.12.001] [PMID] [PMCID]
- Moschak TM, Terry DR, Daughters SB, Carelli RM. Low distress tolerance predicts heightened drug seeking and taking after extended abstinence from cocaine self-administration. Addiction Biology. 2017; 23(1):130-41. [DOI:10.1111/adb.12488] [PMID] [PMCID]
- Forouzanfar A, Gholamali Lavasani M, Shoa Kazemi M. [The effectiveness of group counselling based on acceptance and commitment therapy in distress tolerance and anxiety sensitivity among female substance abusers (Persian)]. Journal of Research on Addiction. 2018; 11(44):101-15. http://etiadpajohi.ir/article-1-1290-fa.html
- Molazadeh J, Ashouri A. [The effectiveness of cognitive-behavioral group therapy in improve-ment of relapse prevention skills and mental health in the addicts (Persian)]. Daneshvar Raftar. 2009; 16(34):1-12. https://www.sid.ir/fa/journal/ViewPaper.aspx?ID=118711
- Jeldkar S, Najafi M, Sotoudeh N. [Effectiveness of group education based on choice theory on increasing the marital flexibility and satisfaction (Persian)]. Journal of Counseling Research. 2014; 13(52):23-36. http://irancounseling.ir/journal/article-1-108-fa.html
- Lombard SJF, Pullen D, Swabey K. Conceptualizing traumafor children of drug addicted mothers: A developmental mapping. Journal of Trauma & Treatment. 2017; 6(1):e1000352. [DOI:10.4172/2167-1222.1000352]
- Nygaard E, Moe V, Slinning K, Walhovd KB. Longitudinal cognitive development of children born to mothers with opioid and poly substance use. The Journal of Pediatric Research. 2015; 78(3):330-5. [DOI:10.1038/pr.2015.95] [PMID] [PMCID]
- Tavakolizadeh J, Nejatian M, Soori A. The effectiveness of communication skills training on marital conflicts and its different aspects in women. Procedia - Social and Behavioral Sciences. 2015; 171:214-21. [DOI:10.1016/j.sbspro.2015.01.112]
- Fooladvand Kh, Borjali A, Hossein Sabet F, Delavar A. [The role of depression, family relationships, and self-efficacy in the prediction of addiction among adolescence (Persian)]. Qom University of Medical Sciences Journal. 2016; 10(3):70-80. http://journal.muq.ac.ir/article-1-850-fa.html
- Fathollahzadeh N, Mirsaififard LS, Kazemi M, Saadati N, Navabi Nejad Sh. [Effectiveness of marital life enrichment based on choice theory on quality of marital relationships and couples’ intimacy (Persian)]. Quarterly of Applied Psychology. 2017; 11(3):353-72. http://apsy.sbu.ac.ir/article/view/19132
- Poorheidari M, Alijani F, Aghayan SS, Keramat F, Masoumi SZ, Asadi Z. [The effect of relationship enrichment training on marital intimacy of infertile couples with domestic violence (Persian)]. Journal of Isfahan University of Medical Sciences. 2016; 34(402):1187-96. http://jims.mui.ac.ir/index.php/jims/article/view/6749
- Aghausofi A, Sharifi Saki S, Ahmadi H, Karimi R. [Effect of enrichment education of communication on conjugal satisfaction of addicted couples (Persian)]. Biannual Journal of Clinical Psychology & Personality (Daneshvar-e-Raftar). 2018; 16(1):49-56. http://cpap.shahed.ac.ir/article_2835.html
- Zywiak WH, Stout RL, Trefry WB, Glasser I, Connors GJ, Maisto SA, et al. Alcohol relapse repetition, gender, and predictive validity. Journal of Substance Abuse Treatment. 2006; 30(4):349-53. [DOI:10.1016/j.jsat.2006.03.004] [PMID]
- Delavar A. [Educational and psychological research (Persian)]. Tehran: Virayesh; 2005. http://opac.nlai.ir/opac-prod/bibliographic/761547
- Alipour A, , Rahimi A, Zare H. [The relationship between mental health and marital satisfaction of married students, Payame Noor University of Tehran (Persian)]. The Journal of Urmia University of Medical Sciences. 2013; 22(7):557-65. http://umj.umsu.ac.ir/article-1-1853-fa.html
Type of Study: Original |
Subject:
Mental Health
Received: 2019/09/2 | Accepted: 2020/02/8 | Published: 2020/10/1
Received: 2019/09/2 | Accepted: 2020/02/8 | Published: 2020/10/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |